The Future of Good Faith Estimates
Change is on the Horizon
 Good faith estimates (GFEs) have been required since 2022, yet the No Surprises Act has drawn relatively little enforcement or new policymaking in this area, with most of the recent energy going into independent dispute resolution. That is likely to change. The momentum behind price transparency, and the Patient Deserves Price Tags Act in particular, suggests action on GFEs is on the horizon. This is the moment to refresh your knowledge and consider how you will position GFEs, because they are going to look very different from how they work today.
Good faith estimates (GFEs) have been required since 2022, yet the No Surprises Act has drawn relatively little enforcement or new policymaking in this area, with most of the recent energy going into independent dispute resolution. That is likely to change. The momentum behind price transparency, and the Patient Deserves Price Tags Act in particular, suggests action on GFEs is on the horizon. This is the moment to refresh your knowledge and consider how you will position GFEs, because they are going to look very different from how they work today.
GFE Versus the Patient Estimation System — A Frequent Confusion
It is easy to conflate a good faith estimate under the No Surprises Act with a patient estimation system under hospital price transparency. While on face value they share a similar aim—helping the consumer understand what they can expect to pay for their healthcare services—they sit under different CMS regulations and ultimately serve different purposes. The table below highlights the key distinctions.
| Consumer Display | Patient Estimation System | Good Faith Estimate | |
|---|---|---|---|
| Which CMS regulation? | Hospital Price Transparency | Hospital Price Transparency | No Surprises Act |
| Consumer or provider facing? | Consumer-facing only | Primarily consumer-facing, optional provider-facing | Facility/provider-facing only |
| Estimate type? | Negotiated rates and discounted cash price | Single out-of-pocket estimate w/ cost-sharing calculations | Itemized expected charges |
| Self-pay or insured? | Both | Both | Self-pay/uninsured* |
| 300 shoppable or all schedulable? | 300 shoppable services | 300 shoppable services | All schedulable |
| Convening and/or co-providers? | Convening only | Convening only | Both |
| Core data needed? | Claims + payer contracts | Claims + payer contracts + cost sharing | Claims + CDM |
*Requirements for GFEs to be sent to insured in-network or out-of-network payers, with advanced EOBs sent to patients, have been delayed.
A few distinctions are worth drawing out. The consumer display is consumer-facing only and, frankly, of limited use. It shows negotiated rates and discount cash prices, not what an insured patient will actually pay. The patient estimation system fills that gap by giving an out-of-pocket figure, lets patients shop independently, and is often used optionally in patient access for upfront collections, though that provider-facing application is not required.
A good faith estimate is different in kind. Patients cannot shop for one; it must be provided orally and in writing by your patient access team, not merely on request, but any time you have a self-pay or uninsured patient with a service scheduled at least three days out. It is itemized, reading almost like a claim, a kind of “pre-claim” sent today to the patient, and it must be all-inclusive, covering expected charges from every provider involved in that patient’s care, not just the convening facility. The patient estimation system, by contrast, needs payer contract data and covers only the convening facility.
Tomorrow’s GFE: A Pre-Claim That Runs Through the Payer
We’ve covered the picture as it stands today, but the future looks materially different. The workflow below shows where GFEs are heading—and why the Patient Deserves Price Tags Act may push to replace the patient estimation system with this process for insured patients.
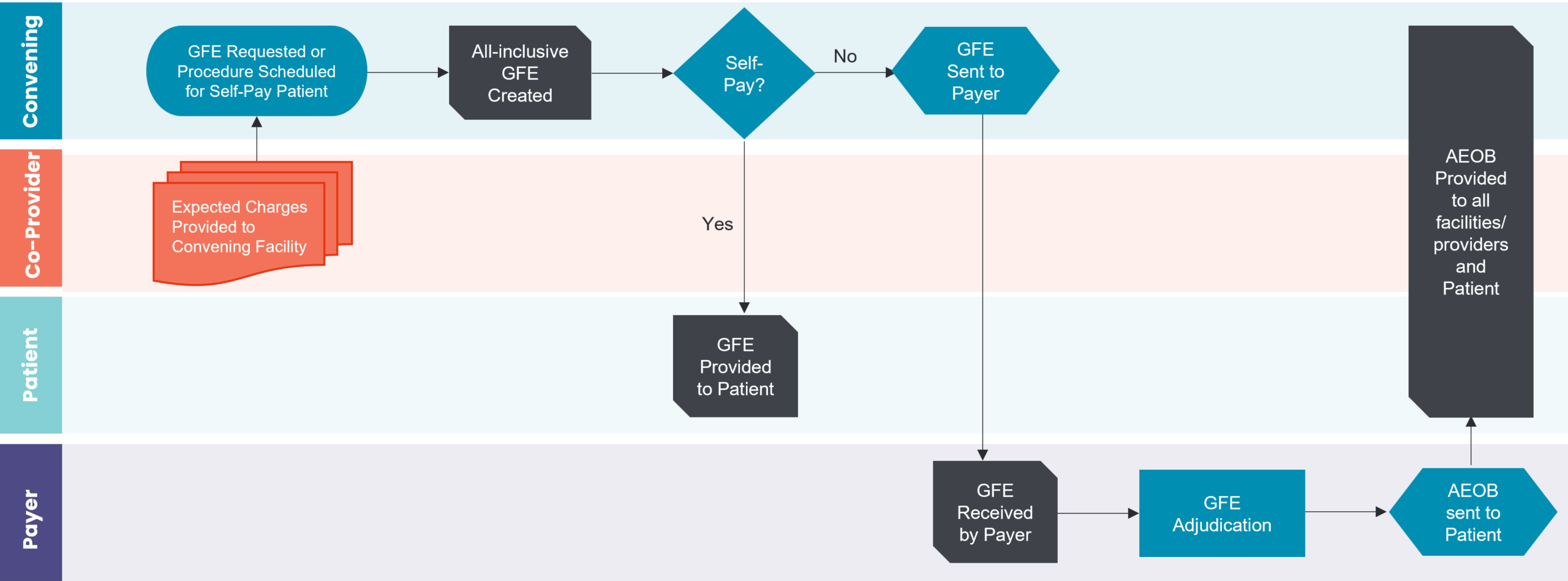
The proposed GFE workflow: expected charges flow from co-providers to the convening facility, and for insured patients the GFE is sent to the payer for adjudication and an Advanced EOB.
When a GFE is requested or a procedure is scheduled, expected charges must be gathered from all providers, convening facility and co-providers alike, and consolidated. For a self-pay patient, the all-inclusive GFE goes to the patient and the process ends. But for an insured patient under the future model, the GFE must be sent to the payer.
This is where the practical problems begin. The industry has not built a clean way to gather expected charges from independent physicians due to HIPAA complications, and there is certainly no standard way to submit this pre-claim or for a payer to accept it. The data-standard transactions (HL7 or otherwise) have not been defined. Beyond that, the payer must adjudicate it: today, they do claims adjudication; under the new model, they would have to perform “GFE adjudication.” This does not have the same ring to it and raises the strange possibility of receiving denials on a free pre-claim. Once adjudicated, the payer would send an advanced EOB to the patient and to all providers and facilities on the GFE.
The advanced EOB is meant to do more than estimate. It should tell the patient whether they are in or out of network. If the patient is out of network, it should list in-network alternatives, with cost-sharing details including the allowed amount, the patient’s out-of-pocket, and what the insurer pays—all delivered before service, with enough time for the patient to decide whether to proceed or cancel.
Time Is of The Essence—and the Math Barely Works
The timing requirement introduces a practical complication. Consider a patient who, on Monday the 13th, schedules a service for Friday the 17th—four days out, satisfying the “three or more days” rule. The patient is self-pay, or insured but choosing not to use coverage. The clock starts immediately.
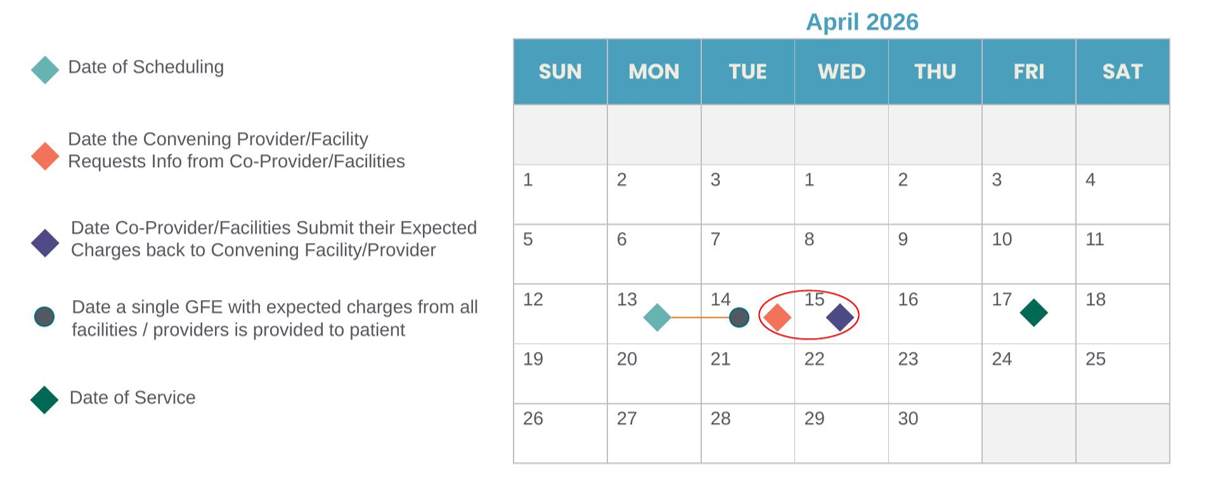
The compressed GFE timeline: from request, co-providers must return expected charges, the convening facility must consolidate, and the patient must receive the GFE at least three days before service.
In that window, the convening facility must collect expected charges from every co-provider, those co-providers must send dollar amounts back, and the consolidated GFE must reach the patient at least three days before service. By the time charges are gathered it is already Wednesday or Thursday—and the three-day-prior requirement has effectively been missed. Short of a time machine, it is not realistic to accomplish this process start to finish in a couple of days. AI and automation may eventually close the gap, but the industry has a long way to go before then. This is an important logistical factor that will have to be resolved before the future-state GFE can work.
Anatomy of a Compliant GFE
Whatever the future holds, the contents of a good faith estimate are well-defined. A compliant GFE includes:
Learn More
Find out how Panacea can enhance your Good Faith Estimates